
Infestation with parasitic worms is the most common disease in many tropical and subtropical countries. These parasitic worms firmly hold the intestinal mucosa and continue their reproduction by egg production. Worms parasitic to man can be categorized as cestodes (tapeworm), nematodes (round worms), and trematodes (flukes). Anthelmintics are the agents which are used to destroy or eliminate these parasitic worms from the gastro intestinal tract. They act by killing or paralyzing the worms so that such worms could be easily expelled out of the gut. Some anthelmintic agents also impair the egg production process in worms. Depending upon the action, anthelmintic agents are categorized into:
- vermifuges or drugs that expel the worms from the body, and
- vermicides or drugs that kill the worms in the body.
Classification
Table of Contents
Presently available anthelmintic agents are structurally diversified. On a chemical basis, they can be classified as
- Phenols
- Chlorinated hydrocarbons
- Antimonial compounds
- Dyes
- Piperazine analogs
- Heterocyclic compounds
- Alkaloids and plant extracts, and
- Miscellaneous agents
(a) Phenolic Anthelmintic Agents
(i) Hexylresorcinol: It is an orally active broad-spectrum anthelmintic agent, originally introduced as a urinary antiseptic. It is particularly effective in the treatment of trichuriasis. It causes tissue irritation and is not used in patients with peptic ulcers. The adult oral dose is 1000 mg once a day.
(ii) Dichlorophen: It is an anthelmintic agent effective in the treatment of tapeworm infections. It detaches the worm from the bowel wall and promotes its digestion in the gut. The adult oral dose is 75 mg/ kg body weight, taken on an empty stomach in the morning. A saline cathartic should be given 2 – 4 hours after the drug to minimize the risk of cysticercosis.
(b) Chlorinated Hydrocarbons
(i) Tetrachloroethylene: It is an unsaturated chlorinated hydrocarbon. It is not used as an anthelmintic agent presently and is now of historical importance only. Presently, it is used only in veterinary practice and in the treatment of fluke infections in humans.
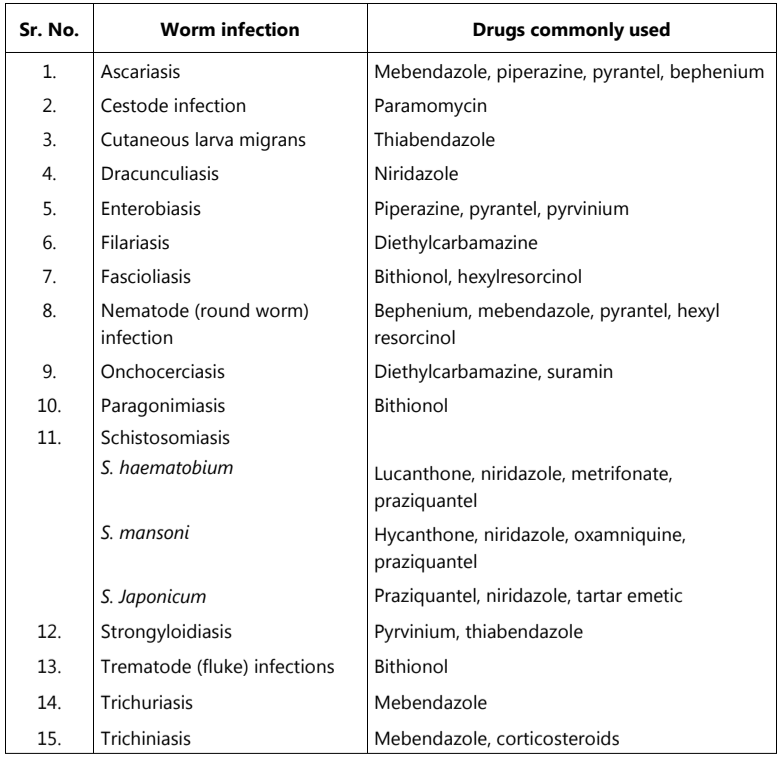
Table 1: Clinically used anthelmintic agents
(c) Antimonial Compounds
These agents are now less favored as anthelmintics because of their high toxicity and difficulty in administration. They exert anthelmintic activity by selectively inhibiting schistosomal phosphofructokinase. This enzyme is necessary to catalyze the conversion of fructose-6-phosphate to fructose-1, 6-diphosphate. Examples include potassium and sodium antimony tartarate. Stibophen is a trivalent effective antimonial leishmanicidal agent with less intensity of adverse effects.
The adult intramuscular dose is 100 mg every second day for 1 – 3 weeks.
(d) Individual Anthelmintic Agents
(i) Thiabendazole: It is an orally active, broad-spectrum anthelmintic agent, effective against a wide range of nematodes. It exerts vermicidal activity specifically against Strongyloides stercoralis, Trichinella spiralis, and Trichiuris trichiura. It acts by deforming the worm eggs. However, the egg count returns to normal if therapy is discontinued. It has no effect on filariasis. It has a plasma half-life of 1.2 hours. It is excreted in the urine mainly as 5-hydroxy thiabendazole either in the form of glucuronide or sulfate. Adverse effects include nausea, vomiting, epigastric distress, anorexia, diarrhea, numbness, skin rash, hyperglycemia, crystalluria, and transient leukopenia.
Thiabendazole is effective in the treatment of A. duodenal (common hookworm), E. vermicularis (pin worm), A. lumbricoides (round worm) and S. stercoralis infections. The adult oral dose is 3 g per day. In early trichinosis, treatment may be continued for 2-3 additional days while in disseminated Strongyloidiasis, treatment may be continued for at least 5 days.
(ii) Diethylcarbamazine: It is an orally active agent belonging to the piperazine category. It acts by sensitizing the microfilaria so that they become plagocytozed by fixed tissue macrophages. It is orally well absorbed and has a plasma half-life of 8 – 12 hours. Upon extensive metabolism, a variety of inactive metabolites are excreted in the urine along with a 10% dose as an unchanged drug.
It is used to treat infections caused by W. bancrofti, W. malayi, and O. volvulus. It is a drug of choice for the treatment of filariasis due to Tetrapetalonema perstans or Tetrapetalonema streptocerca. It may also be used in tropical eosinophilia and Ascaris infections. The adult oral dose is 2 mg/kg body weight three times a day after meals for 1-3 weeks.
(iii) Lucanthone: It is an orally active antischistosomal agent derived from a yellow dye and is effective against S. haematobium. It acts by preventing helmintic ova production or its release. This destroys the parasite. It is less favoured clinically because of its adverse effects. Hycanthone is a hydroxymetabolite of lucanthone. It possesses marked schistosomicidal activity. The adult oral dose is 5 mg/kg two to three times a day for 5 – 10 days in the treatment of schistosomiasis.
(iv) Mebendazole: It is a benzimidazole derivative having broad-spectrum anthelmintic activity. It shows poor oral absorption. About 78 – 80% administered dose is bound to the plasma-proteins. It has a plasma half-life of 2.5-5.5 hours. About 95% dose is excreted unchanged or as 2 – amino – 5 – benzoyl – benzimidazole (primary metabolite) in the faeces. Up to 2 – 5% dose appears in the urine unchanged or as a primary metabolite.
It is effective in the treatment of ascariasis, trichuriasis, and hookworm infections in an oral dose of 100 mg twice a day for 3 days. In enterobiasis, a single oral dose of 100 mg is given. After 2 weeks, the second dose of 100 mg may be given.
(v) Metrifonate: It is an organophosphorus compound that is an inhibitor of the cholinesterase enzyme, and is used as an anthelmintic and agricultural insecticide. It has a plasma half-life of 1.5 hours. It is extensively metabolized by plasma and schistosomal arylesterases. Principal metabolites include dichloro-(2, 2 – dichlorovinyl dimethyl phosphate) and various inactive products.
Adverse effects include nausea, vomiting, colic, abdominal pain, mild vertigo, lassitude, decreased sperm count, and some intestinal nematodes.
It is used for the treatment of urinary schistosomiasis and S. haematobium infections. The adult oral dose is 5-15 mg/kg body weight 3 times after every 2 weeks.
(vi) Niridazole: It is an orally active nitrothiazole derivative having anthelmintic and antibacterial activities. It also exhibits amoebicidal and schistosomicidal activities. Besides this, it is also effective against guinea worm (D. medinensis) infestation.
It undergoes an extensive first-pass hepatic metabolism. 1 – Thiocarbamoyl – 2 – imidazolidinone is the active metabolite. The metabolites appear both, in urine and feces.
It is used in the treatment of D. medinensis. It may also be used for the therapy of schistosomiasis due to S. japonicum.
(vii) Niclosamide: It is a salicylanilide derivative having anthelmintic activity. It is effective only in the treatment of intestinal cestodes. Its oral absorption is poor. Major dose is excreted through the feces.
It is used in the treatment of diphyllobothriasis (Diphyllobothrium latum), Hymenolepiasis (H. nana), Taeniasis (T. saginata) and Dipylidiasis (Dipylidium conium). Enterobium vermicularis is also susceptible. For destruction of tapeworm, niclosamide is the most effective and safe drug.
The adult oral dose is 500 mg usually in the fasting condition 3 – 4 times a day. Antiemetic may be given one hour before and purgative about 2 hours, after the treatment.
(viii) Oxamniquine: It is an orally active yellow dye having anthelmintic activity. Chemically it is 2 – amino methyl tetra-hydroquinoline derivative. It is especially effective against Schistosoma mansoni and has a plasma half-life of 1 – 2.5 hours. Principal metabolites include 6 – carboxyl and 2 – carboxylic acid derivatives which are excreted in the urine along with traces (0.4 – 1.9% dose) of the parent drug.
It is an effective schistosomicidal agent used against Schistosoma mansoni and is also used in combination with metrifonate in the treatment of mixed mansoni and haematobium infections.
Adult oral dose is 15 – 60 mg/kg of body weight as a single dose given at bedtime.
(ix) Pyrvinium Pamoate: It is an organic dye used as an anthelmintic agent. It is not orally absorbed. Major portion of administered dose appears unchanged in the feces. Adverse effects are few and include gastric irritation, photo-sensitization, nausea, vomiting, diarrhea, cramps, and skin rash. It is used in the treatment of enterobiasis caused by pin worm (E. vermicularis).
The adult oral dose is 5 mg (base)/ kg body weight per day.
(x) Suramin: It is a dye derivative having trypanocidal activity. Freshly prepared solutions should always be used for I.V. administration. About 99% administered dose is bound to the plasma proteins. It has a plasma half-life of 48 – 49 days. It does not undergo significant metabolism. About 60% dose appears unchanged in the urine.
It is used in the treatment of African trypanosomiasis and for onchocerciasis either alone or along with arsenical therapy. It is effective in the prophylaxis of Rhodesian and Gambian trypanosomiasis.
Adult I.V. dose is 1 g on days 1, 3, 7, 14, and 21 that is slowly injected in the form of a 10% solution. The therapy may be continued for additional 5 weeks.
(xi) Piperazine citrate: It is an orally active anthelmintic agent available as citrate, phosphate, or adipate salt form. It is effective against Ascaris lumbricoides and Enterobium vermicularis (oxyuriasis). The major dose fraction appears unchanged in the urine.
It is used in the treatment of oxyuriasis. A single daily dose of 65 mg/kg of body weight may be given for a week. The dose schedule may be repeated after 15 days. It may also be used in the treatment of combined ascariasis and oxyuriasis.
(xii) Bephenium hydroxynaphthoate: It is a quaternary ammonium salt previously designed to treat hookworm infections. It is poorly absorbed from GIT. It is used to treat infections caused by Ascaris lumbricoides, Trichostrongylus orientalis, and ternideniasis. It is excreted in urine only in trace amounts.
The adult oral dose is 5 g twice a day with an empty stomach for 3 – 7 days.
(xiii) Bithionol: It is a phenolic anthelmintic agent used for the treatment of paragonimiasis and fascioliasis. Adverse effects includes nausea, vomiting, diarrhea, colic, urticaria, and photodermatitis. The adult oral dose is 50 mg/kg of body weight every second day for ten doses.
(xiv) Chloroquine: It is an orally effective 4-aminoquinoline antimalarial agent which may be used in the treatment of clonorchiasis. It acts by depressing ova output. It does not exert a vermicidal effect.
(xv) Pyrantel pamoate: It is a poor orally absorbed broad-spectrum anthelmintic and neuromuscular blocking agent. It is effective against infections with hook-worm, pinworm, and round-worm. About 60 – 70% dose appear in the faeces in an unchanged form. Inactive metabolites appears in the urine along with a 10 – 20% dose in unchanged form. It is contraindicated during pregnancy and in children less than 2 years of age.
It is effective in the treatment of ascariasis, enterobiasis, ancylostoma, Necator americanus and Trichostrongylus. It may be used alongwith oxantel to treat mixed infections with Trichuris trichiura. Adult oral dose is 11 mg/kg to a maximum of 1 g per day. Treatment may be repeated, if necessary after two weeks.
In general, various anthelmintic agents exert their activity by producing toxic effects on both, the gastrointestinal tract and the parasitic worms. They induce contraction of the worms which is followed by their tonic paralysis. Thereafter the worms are removed by the peristaltic movement of smooth muscles of GIT that helps to excrete out these parasites in the feces. Metrifonate, an organophosphorus inhibitor of cholinesterase enzymes, produces rapid and almost complete inhibition of cholinesterases in the worms. Of course, the drug, to a certain extent, also affects the host due to its cholinesterase-inhibitory activity.
Depending upon the type of worm involved, anthelmintic agents are used alone or in combination with each other. For example, in tapeworm infections, niclosamide is a drug of choice. In nematode infections, piperazine, mebendazole, and pyrantel palmitate are used because of their broad spectrum of anthelmintic activity. For filaria, diethylcarbamazine is generally used, while in trematode infections, niridazole, bithionol, and oxamniquine are effective agents.
Chemotherapy of Parasitic Diseases
At least 45,000 species of protozoa have been described, out of which many species are parasitic. Examples of such parasitic species include, single-celled protozoa, amoeba; helminthes etc. Parasitic infections pose a major world-wide health problem. Moreover, the development of resistance by these parasites to drugs and mosquitoes to insecticides, makes the problem more complicated. Many factors contribute to the spread of these parasitic diseases.
Table 2: Commonly occurring parasitic diseases
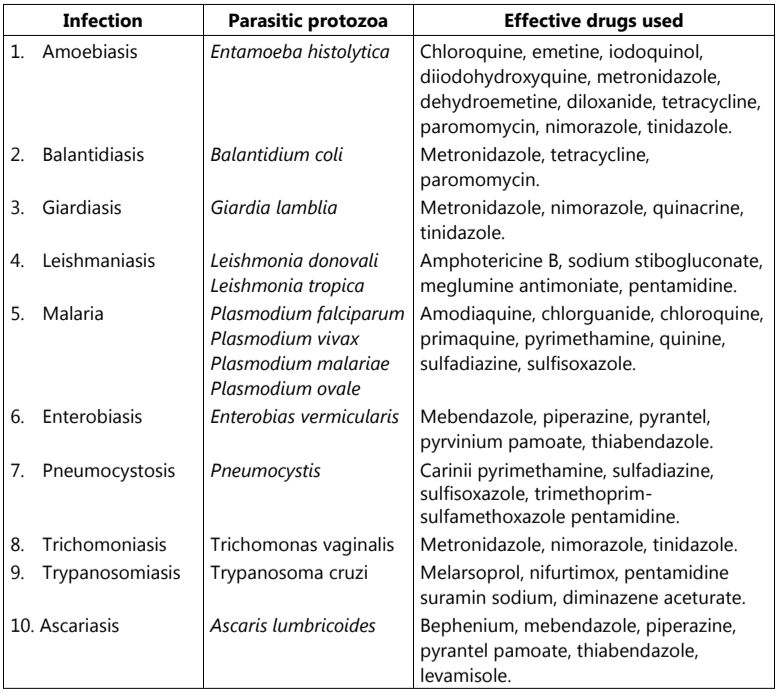
Infections with helminthes and protozoa are the most common causes of human diseases. The occurrence of these infections is much more in poor, undeveloped, or developing countries than in developed countries. Population crowding, poor sanitation, and negligence to provide health education are some of the important contributing factors. These diseases are prominently seen in tropical countries.
Parasitic diseases are easy to acquire, difficult to eradicate, and prone to relapse. Table 2 illustrates commonly occurring parasitic diseases.
Make sure you also check our other amazing Article on : What are Antifungal Agents?