Asthma is a chronic inflammatory disorder of the airways associated with a variable (usually reversible) airflow obstruction and enhanced bronchial hyperresponsiveness to a variety of stimuli.
Causes of Asthma:
Table of Contents
Asthma is characterized by excessive sensitivity of the lungs to various stimuli. There is increasing evidence to suggest genetics play an important role in the etiology of the disease.
Environmental factors interact with inherited factors to increase the risk of asthma. Environmental triggers range from viral infections and allergies to irritating gases and particles in the air. Each person reacts differently to the factors that may trigger asthma.
Physiological factors that may trigger or increase asthma symptoms include:
- Viral upper respiratory infections.
- Heavy exercise.
- Untreated conditions such as rhinitis, sinusitis, and gastroesophageal reflux (GERD).
- Drugs: NSAIDs such as aspirin.
- Ibuprofen, acetaminophen, naproxen sodium, and Ketoprofen; statin drugs (cholesterol-reducing medications) and other anti-inflammatory drugs.
- Stress and strong emotions.
- Menstrual cycle/hormone changes.
Common indoor environmental irritants and allergens that can trigger asthma symptoms or an asthma attack include:
- Pet fur or feathers, pet urine, saliva, and dander.
- House-dust mites.
- Cockroach waste and decomposed bodies of dead animals.
- Mold and mildew spores. (leaking plumbing, leaking roof, etc.)
- Tobacco smoke and wood smoke.
- Perfumes, hairsprays, scented lotions, and cologne.
- Air fresheners, incense sticks, and scented candles.
- Cleaning solutions, pesticides, and paint fumes.
Common outdoor environmental irritants and allergens that can trigger asthma symptoms or an asthma attack include:
- Pollen from trees, grasses, and weeds.
- Mold and mildew spores. (wet rotting leaves on the ground)
- Changes in humidity (high humidity).
- Exposure to cold air or hot humid air.
- Industrial emissions, vehicle or truck exhaust, and other air pollutants such as coal dust.
- Ozone: [O3] is a highly reactive form of oxygen that results from sunlight mixing with hydrocarbons (also called volatile organic compounds) and nitrogen oxides released in fuel combustion)
Food Allergy:
Food allergies involve the body’s immune system reacting to proteins found in food. The body treats these proteins the same way as it would be a disease. Different people react to different types of food although some types have a greater chance of becoming a trigger. Between 2% to 10% of people are affected by food allergies, with a greater percentage occurring in children. Reactions can occur within a few minutes or over several hours. Undiagnosed and untreated, severe attacks can be fatal.
Based upon causes, asthma is divided into two types:
a. Intrinsic asthma: Usually develop beyond age 40 and have many causes other than exposure to allergens.
b. Extrinsic asthma: Most commonly develop in childhood and is caused by exposure to definite allergens.
Classification of Asthma:
The current classification of asthma is based on clinical severity. This allows asthma sufferers and clinicians to better manage treatment choices and clinical outcomes.
1. Mild Intermittent Asthma: It occurs in people with daytime symptoms that occur no more frequently than twice a week and night-time symptoms that occur no more than twice a month. These people are usually asymptomatic with a normal Peak Expiratory Flow Rate between exacerbations. Exacerbations vary in intensity but are usually brief, lasting only hours to days. They do not take daily medications for long-term control, only short for quick relief.
2. Mild Persistent Asthma: It is characterized by daytime symptoms that occur more than twice a week but less than once a day with night-time symptoms more frequently than twice a month. These people are asymptomatic but have abnormal pulmonary function tests. Exacerbations begin to limit their activity. They usually take one medication daily for long-term control. Using medications for quick relief daily indicates a need for additional long-term therapy.
3. Moderate Persistent Asthma: It occurs in people who have daytime symptoms every day and night-time symptoms more than once a week. Exacerbations limit their activity and occur at least twice a week, and may last for several days. These individuals take one or two long-term control medications. Also using medications for quick relief daily indicates a need for additional long-term therapy.
4. Severe Persistent Asthma: It is characterized by continual daytime symptoms and frequent night-time symptoms. They experience limited physical activity and exacerbations are frequent. These people often take two medications daily for long-term control. Also using medications for quick relief daily indicates a need for additional long-term therapy.
Pathophysiology of Asthma:
The various common allergens are pollens, dust, mites, some food material, and certain drugs which precipitate the asthmatic attack. The allergens upon exposure stimulate the production of IgE which further bind to mast cells. Upon re-exposure to the same allergen, the said allergens readily bind to IgE and result in degranulation of mast cells to release certain inflammatory mediators such as histamine, leukotrienes, prostaglandins, etc.
In a response to the above changes, WBC’s migrated into the area to engulf the allergens. The phagocytic reaction causes the release of basic proteins which are lytic agents for tissue and further promote inflammation.
With exposure to a trigger, a cascade of cellular responses cause:
- Increased production of thick tenacious mucus with impaired mucociliary function.
2. Mucosal swelling due to increased vascular permeability and vascular congestion.
3. Bronchial smooth muscle contraction
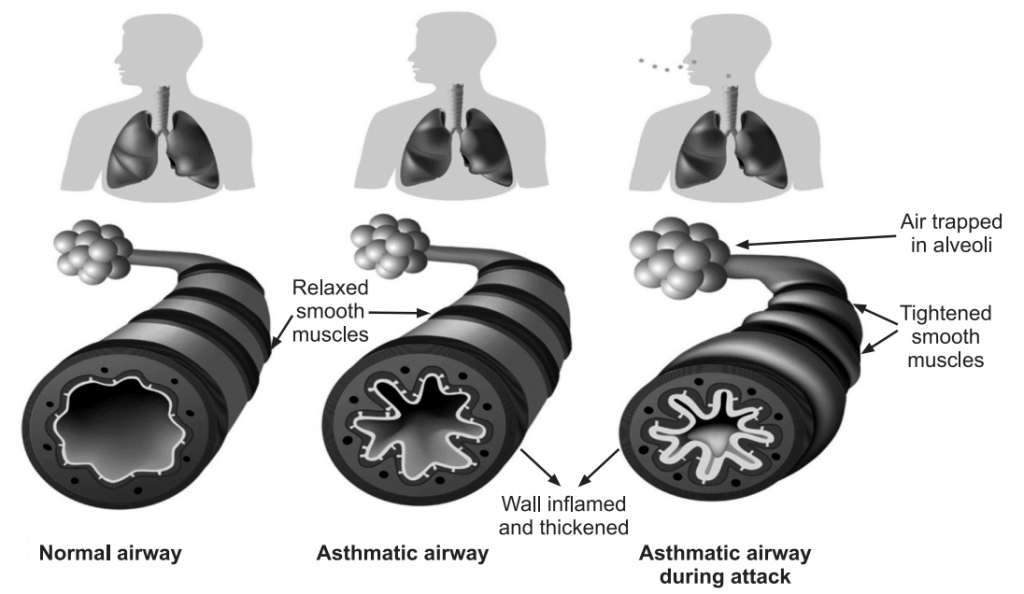
4. These changes cause bronchial hyperresponsiveness and obstruction. Airway obstruction increases resistance to airflow and decreases flow rates, including expiratory flow. Impaired expiration causes hyperinflation distal to the obstruction and increases the work of breathing. These changes are not uniform throughout the lungs but regional. Continued air trapping causes increased intrapleural and alveolar gas pressures resulting in decreased perfusion of the alveoli, the result is hypoxia.
5. Late Asthma Response occurs in cases of significant allergen exposure. The symptoms can recur 4 to 12 hours after the initial attack due to persistent cellular activation. It can be more severe than the initial attack.
6. Untreated inflammation can cause long-term irreversible airway damage (airway remodeling).
Symptoms of Asthma:
Asthma affects the airways, causing them to tighten, become inflamed, or fill with mucus. Asthma symptoms can range from mild to severe. Most people will only experience occasional symptoms, although a few people will have problems most of the time and include:
- Coughing, especially at night, during exercise, or when laughing.
- Shortness of breath.
- Chest tightness.
- Wheezing (a whistling or squeaky sound in the chest when breathing, especially while exhaling).
- Any asthma symptom is serious and can become deadly if left untreated.
- Symptoms may be triggered by exposure to an allergen (such as ragweed, pollen, and pet hair or dust mites), irritants in the air (such as smoke, chemical fumes, or strong odors), or extreme weather conditions.
Diagnosis of Asthma:
Exacerbations of asthma symptoms equate to an individual’s control of their asthma. To prevent long-term complications of airway remodeling, early detection with an accurate diagnosis is needed to exclude other diseases and causes for difficulty breathing. For example, Chronic obstructive pulmonary disease, Congestive heart failure, Pulmonary embolisms, or mechanical obstruction (from tumors).
An asthma diagnosis is based on several factors, including a detailed medical history, a physical exam, symptoms, and overall health, and test results.
Medical History and Physical Examination:
The first step in diagnosing asthma is to look for signs of asthma or allergies. These signs include wheezing (high-pitched whistling sounds when breathing out) and a runny nose or swollen nasal passages, and allergic skin conditions (such as eczema).
Lung Function Tests:
Lung function tests are asthma tests that assess lung function. The two most common lung function tests used to diagnose asthma are spirometry and methacholine challenge tests.
Asthma and COPD (Chronic Obstructive Pulmonary Disease) causes problems by narrowing the bronchial tubes (or airways), resulting in shortness of breath. Narrowed airways are difficult to breathe through. The greater the narrowing, the more difficult breathing becomes.
Spirometry:
It is a simple breathing test that is of great value for measuring exactly how many bronchial tubes have narrowed. A spirometer measures the amount (volume) and speed (flow) of air that can be inhaled and exhaled, indicating how well lungs are performing. It is often used to determine the amount of airway obstruction. This enables to make decisions about lung condition and to plan the best asthma treatment.
Methacholine Challenge Test:
This lung function test for asthma is more commonly used in adults than in children. It might be performed if symptoms and screening spirometry do not clearly or convincingly establish a diagnosis of asthma. Methacholine is an agent that, when inhaled, causes the airways to spasm (contract involuntarily) and narrow if asthma is present. A methacholine challenge test is a type of bronchoprovocation test, which measures lung function after exposure to factors that commonly trigger wheezing and other asthma symptoms.
The purpose of the Methacholine Challenge Test is:
- To identify bronchial hyperresponsiveness in people who have normal results on standard pulmonary function tests.
- To diagnose mild asthma in some atypical cases, such as persistent cough
- To diagnose occupational (workplace) asthma caused by certain dust or chemicals.
- To help determine the risk of developing asthma, evaluate asthma severity and assess response to asthma treatment.
- To evaluate the effectiveness of asthma medications and determine the risk for developing asthma in the future.
Exhaled Nitric Oxide Test:
It is a quick and easy way to measure inflammation (swelling) in the bronchial tubes of the lungs. During inflammation, higher than normal levels of nitric oxide (NO) are released from epithelial cells of the bronchial wall. The concentration of NO in exhaled breath, or fractional exhaled nitric oxide (FeNO), can help to identify airway inflammation, and thereby support a diagnosis of asthma when other objective evidence is lacking.
Allergy Tests:
Allergy skin tests are vital in finding out whether asthma is due to inhalant allergens. Drops of several allergen extracts are placed on the skin (usually the forearm) and the skin is pricked lightly through the drops. A positive reaction will cause some itching and a bump at the site within 10 minutes.
A blood test for allergic antibodies to various allergens is an alternative but in some cases can be less likely to detect an allergy than skin tests.
Prevention and Treatment of Asthma:
Prevention of exposure to known triggers is warranted. Hyposensitization may be beneficial if asthma has an allergic mechanism, in such cases:
- Identify and avoid asthma triggers.
- Identify and treat attacks early and monitor breathing.
- Other measures include a dust-free house.
- Intake of selective type of food.
- Avoid exposure to extreme cold conditions.
- Get vaccinated for influenza and pneumonia.
Pharmacological Treatment:
Drug therapy depends on the frequency and severity of attacks. The bronchodilators are often considered rescue inhalers, while the other medications are considered more prophylactic or therapeutic medications.
1. Bronchodilators (Sympathomimetics):
The mechanism of action for sympathomimetic bronchodilators is to bind the receptors in airway smooth muscle thus causing bronchodilation and increased ciliary beat frequency. e.g. Albuterol, Salbutamol, and Terbutaline.
2. Anticholinergic agents:
The effect of anticholinergic bronchodilators is bronchodilation through inhibition of bronchoconstriction secondary to blockade of the effects of acetylcholine. The mechanism of action for anticholinergic bronchodilators is non-selective antagonism of muscarinic receptors leads to downregulation of cGMP which results in bronchodilation. Additional acetylcholine is released in response, thus overcoming the effect in smooth muscle. e.g. Ipratropium, Aclidinium.
3. Corticosteroids:
The effect of inhaled corticosteroids is reduced airway inflammation. Overall airway bronchial hyper-responsiveness decreases. Improved asthma control and increased sensitivity of β-receptors in smooth muscle. The mechanism of action for inhaled corticosteroids is to suppress granuloma formation, reduce arachidonic acid metabolism, up-regulate β-adrenergic receptors on leukocytes, and decrease the synthesis of prostaglandins and leukotrienes. e.g. Beclomethasone, Flunisolide, Triamcinolone.
4. Biologic Response Modifiers (Monoclonal Antibodies):
The effect of Biologic Response Modifiers is decreased frequency of allergen-induced asthma exacerbations. The mechanism of action for Biologic Response Modifiers is, when the monoclonal antibody binds to IgE, interferes with mast cell binding. This prevents mast cell degranulation and the release of inflammatory mediators. Cytokine release seen in the late phase of an allergic reaction is also prevented by blocking the receptors on dendritic cells, epithelial cells, eosinophils, monocytes, and platelets. E.g. Omalizumab.
5. Leukotriene Receptor Antagonists:
The effect of leukotriene receptor antagonists in the prevention of allergen-induced bronchoconstriction. The mechanism of action for leukotriene receptor antagonists is antagonism of cysteinyl-leukotriene receptors, thus preventing histamine release. e.g. Montelukast and Zafirlukast.
6. Mast Cell Stabilizers:
The effect of mast cell stabilizers is the prevention of bronchoconstriction and inflammation. The mechanism of action of mast cell stabilizers is to antagonize mast cell degranulation to prevent the release of histamine and other mediators of allergic reaction. Agents do not interfere with IgE. The anti-inflammatory mechanism is unknown. e.g. Cromolyn and Nedocromil
7. Methylxanthine Derivatives:
The mechanism of action for methylxanthine derivatives is bronchodilation. The mechanisms of action include prostaglandin antagonism, stimulation of endogenous catecholamines, inhibition of calcium influx into smooth muscle (preventing muscle contraction), antagonism of adenosine receptors, and inhibition of release of mediators from leukocytes and mast cells. E.g. Theophylline.
Make sure you also check our other amazing Article on : Respiratory System