INTRODUCTION
Table of Contents
Drugs acting on the uterus are uterine stimulants and uterine relaxants.
These drugs directly can affect the endometrium and myometrium. Important drugs affecting the endometrium and myometrium are estrogens and progesterone.
Myometrium receives both sympathetic and parasympathetic innervations. So autonomic drugs can affect motility.
Drugs affecting directly and indirectly moderately affect the normal and gestational status of the uterus.
UTERINE STIMULANTS
These drugs increased uterine motility so they are called Ecbolics/ Abortifacients/ Oxytocics.
Oxytocin
- Oxytocin is a powerful hormone. Oxytocin’s level increases when, we hug, or kiss someone. It plays roles especially in sexual reproduction, the most common situations are before and after childbirth.
- It is released in large amounts after distension of the cervix and uterus during labor, facilitating birth, maternal bonding, and after stimulation of the nipples, breastfeeding.
- This hormone affects orgasm, social recognition, pair bonding, anxiety, and breastfeeding. That’s why sometimes it is called the “love hormone”.
- Oxytocin is produced in the hypothalamus. The myoepithelial cells of the breast, which surround the alveoli of the mammary gland, and the smooth muscle cells of the uterus.
- Oxytocin is controlled by a positive feedback mechanism where the release of the hormone causes an action that stimulates more of its release. When contraction of the uterus starts, for example, oxytocin is released which stimulates more contractions and more oxytocin to be released. In this way, contractions increase in intensity and frequency.
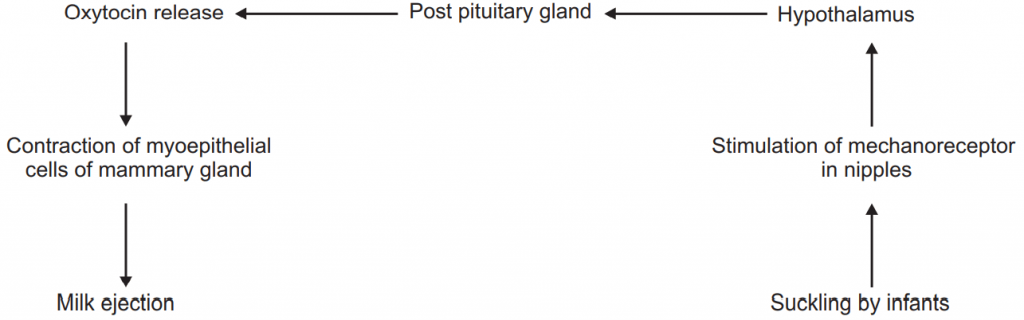
- There is also positive feedback involved in the milk-ejection reflex. When a baby sucks at the breast of its mother, the stimulation leads to oxytocin secretion into the blood which then causes milk to be let down into the breast. Oxytocin is also released into the brain to help stimulate further oxytocin secretion. These processes are self-limiting; production of the hormone is stopped after the baby is delivered or when the baby stops feeding.
- Oxytocin is a mammalian hormone that has many functions, the most notable having to do with pregnant or lactating mammals. In this capacity, some of the hormone’s main functions are preparing a female’s body for childbirth.
- Oxytocin as feed inhibitor, maintaining homeostasis In consummatory behavior.
- The structure of the hormone is very similar to that of vasopressin, also a nonapeptide with a sulfur bridge, whose sequence differs from oxytocin by two amino acids.

Classifications:
- Posterior Pituitary Hormone: Oxytocin.
- Ergot Alkaloids: Ergometrine, Methyl Ergometrine.
- Prostaglandin: PGE2, PGF2α, Misoprostol.
- Miscellaneous: Quinine, Ethacridine.
Oxytocin means: OXYS-Quick; TOKOS-Child Birth.
- It is a nonapeptide hormone derived from the paraventricular nucleus of the hypothalamus and released from the posterior pituitary gland along with ADH.
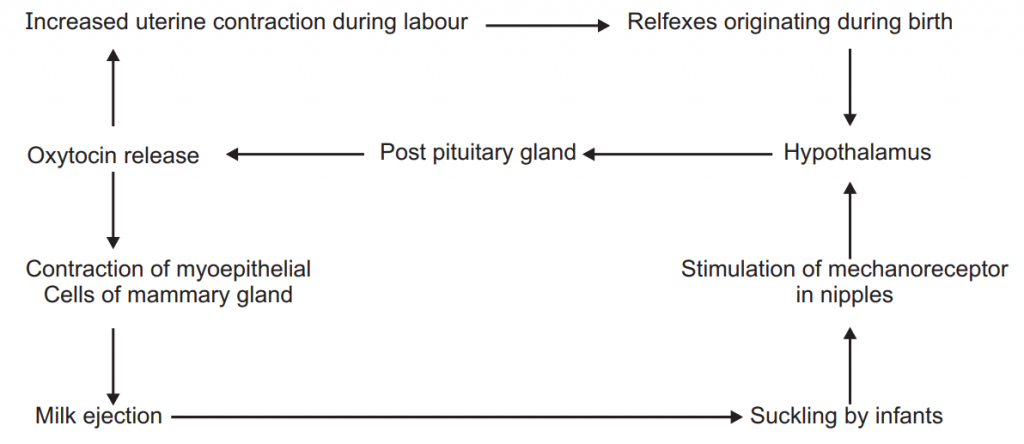
Flowchart of Mechanism and Pharmacological actions of Oxytocin and factors controlling Oxytocin release:
- Oxytocin acts on Oxytocin receptors which are mediated by:
(a) It acts through the IP3 /DAG system and increased the influx of Ca2+ release, which causes contraction.
(b) Caused depolarization.
(c) Increased PG synthesis and release by endometrium which causes contraction.
(d) All the above actions together cause Uterine contraction.
Pharmacological Actions:
Uterus:
- Oxytocin increases the force and frequency of uterine contraction.
- The basal tone of the uterus is also increased at a high dose.
- At a low dose, there is relaxation in between the contraction.
- Increased uterus contraction is due to heightened electrical activity of the myometrium.
Breast:
- It causes contraction of myoepithelial cells surrounding the mammary gland, leads to 2the milk ejection.
CVS:
- Promotes Oxytocin release, which leads to vasodilatation and decreased BP.
Kidney:
- High dose decreases urine output.
ADME:
- Being peptide is inactivated by the oral route of administration. So it is administered by the parenteral/intranasal route. Rapidly degraded in liver and kidney by oxygenase enzyme and excreted in the urine.
Therapeutic activity:
- Induction of labor.
- In uterine inertia.
- Postpartum hemorrhage.
- Cesarean section.
- Abortion.
- Breast engorgement and milk ejection.
ADR:
- Due to powerful contraction during delivery, it may cause damage to the soft tissue of the mother and baby.
- Asphyxia and Death.
Ergometrine
MOA:
- It acts through the IP3 /DAG system and increased the influx of Ca2+ release, which causes contraction.
- Caused depolarization.
- Increased PG synthesis and release by endometrium which caused contraction.
- All the above actions together caused uterine contraction.
Pharmacological Actions:
Uterus:
- It increases the force and frequency of uterine contraction.
- The basal tone of the uterus is also increased at a high dose.
- At a low dose, there is relaxation in between the contraction.
- Increased uterus contraction is due to heightened electrical activity of the myometrium.
CVS:
- Weaker vasoconstrictor, cause an insignificant rise in BP.
GIT:
- At high dose increased GIT peristalsis.
ADME:
- Well absorbed and distributed well, Metabolised in the liver, and excreted in the urine.
Therapeutic Uses:
- Management of the third stage of pregnancy.
- To control and prevent postpartum hemorrhage.
- To ensure normal ovulation.
ADR:
- Due to powerful contraction during delivery, it may cause damage to the soft tissue of the mother and baby.
UTERINE RELAXANTS
- The primary role of uterine relaxants is to prevent pre-mature delivery or labor that starts before the end of the 37th week of gestation.
- Premature labor can be developed spontaneously or may follow genetically predisposed to early rupture of fetal membrane.
- Tocolytics agents either act directly to suppress myoepithelium smooth muscle contraction by decreasing intracellular Ca2+ concentrations and reducing the efflux of Ca2+ on muscle contraction.
- Or they may act indirectly by inhibiting the synthesis or release or receptor actions of PG or Oxytocin.
- These drugs are also used to delay labor, arrest threatened abortion, or treat dysmenorrheal.
- Suppression of labor also important to allow the fetus to mature to initiate glucocorticoid therapy to mother so that the lungs of the newborn baby get sufficient time for maturation and neonatal respiration distress can be reduced.
- Tocolytics agents use for this purpose are β adrenoreceptor agonists, magnesium sulfate, Ca2+ channel blocker, hydroxyl progesterone, PG synthesis inhibitors, and Oxytocin receptor antagonists.
Classifications:
- Selective β adrenoreceptor agonists- Ritodrine, Salbutamol, Terbutaline, Orciprenaline, Isoxsuprine.
- Calcium Channel blocker: Verapamil, Nifedipine, Nicardipine, Amlodipine.
Ritodrine:
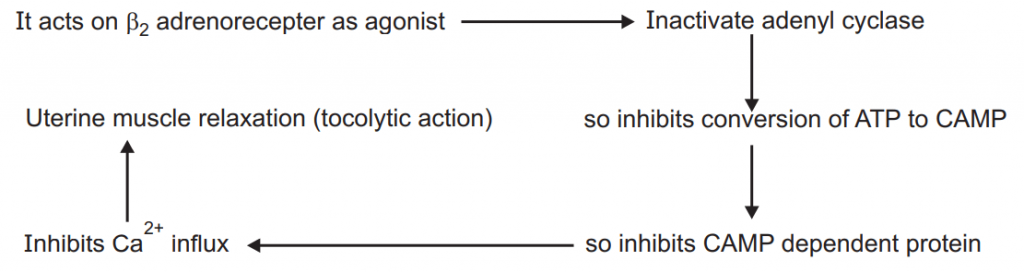
MOA:
Therapeutic uses:
- Uterine relaxants.
ADR:
- Hypotension, Bradycardia, Arrthymia, Pulmonary edema, Hypokalamia, Hyperglycemia.
Calcium Channel Blockers:
MOA:
- Calcium Channel Blockers block L-Type of voltage-gated calcium channel in the myometrium.
↓
Inhibits Calcium influx
↓
Uterine muscle relaxation (Tocolytic action)
Therapeutic uses:
- Uterine relaxants.
ADR:
- Hypotension, Bradycardia, Foetal hypoxia.
Magnesium Sulphate:
MOA:
- It directly uncouples the excitation coupling and inhibits cellular action potential.
- Cause relaxation of uterine muscles, tocolytic action.
- It is preferred over β2 agonists if the patient is having cardiac and hyperthyroidism problems.
Therapeutic uses:
- Uterine relaxants.
ADR:
- Feeling of warmth, sweating, flushing, dry mouth, nausea, headache, palpitation.
Make sure you also check our other amazing Article on : Oral Contraceptives