Introduction:
Healing:
Table of Contents
Tissue injury may result in cell death and tissue destruction. Healing on the other hand is the body response to injury in an attempt to restore normal structure and function. The process of healing involves two distinct processes:
Regeneration: When healing takes place by the proliferation of parenchymal cells and usually results in complete restoration of the original tissues.
Repair: When the healing takes place by the proliferation of connective tissue elements resulting in fibrosis and scarring.
These two processes take place simultaneously.
1. Regeneration:
Some parenchymal cells are short-lived while others have a long life span. To maintain the proper structure of tissue, these cells are under the constant regulatory control of their cell cycle. These include growth factors such as epidermal growth factor, fibroblast growth factor; platelet-derived growth factor, and endothelial growth factor.
Regeneration of any type of parenchymal cell involves the following two processes.
- The proliferation of original cells forms the margin of injury with migration to cover the gap.
- The proliferation of migrated cells with subsequent differentiation and maturation to reconstitute the original tissue.
Depending upon their capacity to divide, cells of the body can be divided into three groups.
1. Labile cells:
These cells continue to multiply throughout life under normal physiologic conditions. These include surface epithelial cells of the epidermis, alimentary tract, respiratory tract, urinary tract, vagina, cervix, uterine endometrium, hematopoietic cells of bone marrow, and lymph node cells spleen.
2. Stable cells:
These cells decrease or lose their ability to proliferate after adolescence but retain the capacity to multiply in response to stimuli throughout adult life. These include parenchymal cells of organs like the liver, pancreas, kidneys, adrenal, and thyroid. Mesenchymal cells like smooth muscle cells, fibroblasts vascular endothelium bone, and cartilage cells.
3. Permanent cells:
These cells lose their ability to proliferate around the time of birth. These include neurons, skeletal muscle, and cardiac cells.
2. Repair:
Repair is the replacement of injured tissue by fibrous tissue. These responses take place by the participation of mesenchymal cells (consisting of connective tissue, stem cells fibrocytes, and histocytes). The process of repair involves:
I. Granulation tissue formation
II. Contraction of wounds.
1. Granulation Tissue Formation:
The term granulation tissue derives its name from the slightly granular and pink appearance of the tissue. Each granule corresponds histologically to the proliferation of new small blood vessels which are slightly lifted on the surface by the covering of fibroblasts and young collagen. The following three phases are observed in the formation of granulation tissue.
a. Phase of inflammation: Following trauma, blood clots at the site of injury. There is an acute inflammatory response with exudation of plasma, neutrophils, and some monocytes within 24 hours.
b. Phase of clearance: Combination of proteolytic enzyme liberated from neutrophils autolytic enzymes from dead tissue cells and phagocytic activity of macrophages clear off the necrotic tissue, debris, and red blood cells.
c. Phase of growths of granulation tissue: This phase consists of two main processes.
(i) Angiogenesis: Formation of new blood vessels at the site of injury takes place by the proliferation of endothelial cells from the margins of several blood vessels. Initially, the proliferated endothelial cells are solid buds but within a few hours develop into the lumen and start carrying blood. The newly formed blood vessels are leakier, accounting for the edematous appearance of new granulation tissue. Soon these blood vessels differentiate into muscular arterioles, thin-walled venules, and true capillaries.
(ii) Fibrogenesis: The newly formed blood vessels are present in an amorphous ground of the surface matrix. The new fibroblasts originate from fibrocytes as well as the mitotic division of fibroblasts. Some of these fibroblasts have a combination of morphologic and functional characteristics of smooth muscle cells.
Collagen fibril begins to appear by about the 6th day. As maturation proceeds, more and more collagen is formed while the number of active fibroblasts and new blood vessels decreases. This results in the formation of inactive looking scar.
2. Contraction of Wounds:
The wound starts contracting after 2-3 days and the process is completed by the 14th day. During this period the wound is reduced by approximately 80% of its original size. A contracted wound results in rapid healing since the lesser surface area of the injured tissue has to be replaced.
In order to explain the mechanism of wound contraction, several factors have been proposed.
1. Dehydration as a result of removal of fluid by drying of the wound was first suggested but without being substantiated.
2. Contraction of collagen was thought to responsible for contraction but wound contraction proceeds at a stage when the collagen content of granulation tissue is very small.
3. Discovery of myofibroblasts appearing inactive granulation tissue has resolved the controversy. These cells have features intermediate between those of fibroblasts and smooth muscle cells. Their migration into the wound area and their active contraction decrease the size of the defect.
Wound Healing:
Healing of skin wounds provides a classical example of the combination of regeneration and repair described above. Wound healing can be accomplished in one of the following two ways:
- Healing by the first intention
- Healing by second intention
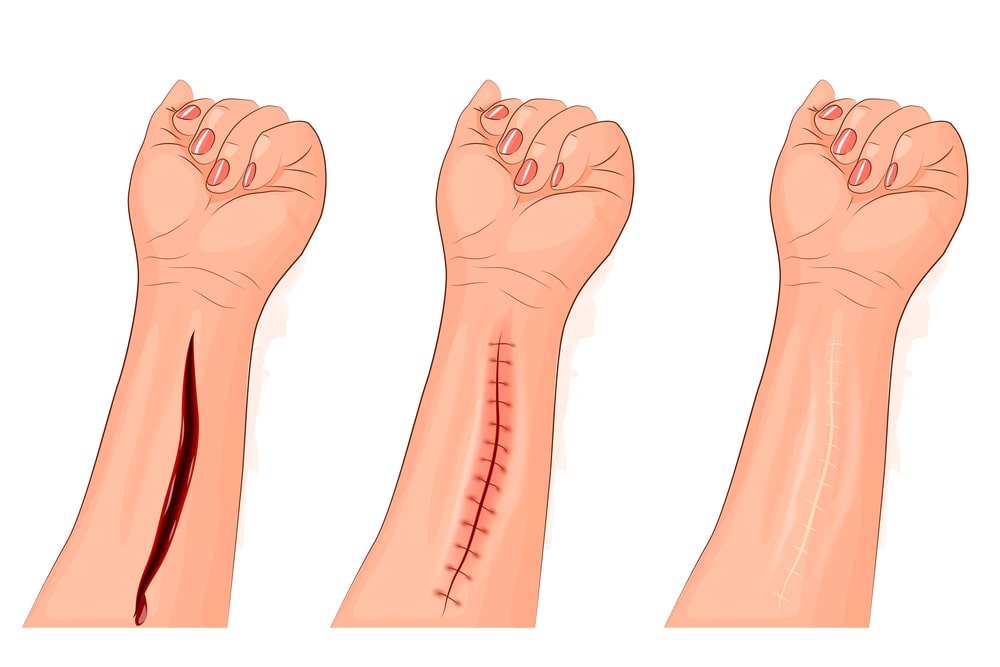
1. Healing by the first intention:
One of the simplest examples of wound repair is the healing of a clean, uninfected surgical incision approximated by surgical sutures. This is referred to as healing by the first intention. The incision causes only focal disruption of epithelial basement membrane continuity and death or a relatively few epithelial and connective tissue cells.
As a result, epithelial regeneration predominates over fibrosis. The narrow incisional space rapidly fills with fibrin-clotted blood; dehydration at the surface produces a scar to cover and protect the healing repair site.
On day first, neutrophils are seen at the incision margin, migrating toward the fibrin clot. Basal cells at the cut edge of the epidermis begin to exhibit increased mitotic activity. Within 24 to 48 hours, epithelial cells from both edges have begun to migrate and proliferate along with the dermis, depositing the basement membrane component as they progress. The cells meet in the midline beneath the surface scab, yielding the thin but continuous epithelial layer.
On days two to three neutrophils have been largely replaced by macrophages, and granulation tissue progressively invades the incision space. Collagen fibers are now evident at the incision margins, but these are vertically oriented and do not bridge the incision. Epithelial cell proliferation continues, yielding a thickened epidermal covering layer.
On days 4 to 5 neovascularization reaches its peak as granulation tissue fills the incisional space. Collagen fibrils become more abundant and begin to bridge the incision. The epidermis recovers its normal thickness as differentiation of surface cells yields a mature epidermal architecture with surface keratinization.
In the second week, there is continued collagen accumulation and fibroblast proliferation. The leukocyte infiltrates, edema, and increased vascularity are substantially diminished. The long process of blanching begins, accomplished by increasing collagen deposition within the incisional scar and the regression of vascular channels.
In the first month, the scar comprises a cellular connective tissue largely devoid of inflammatory cells and covered by an essentially normal epidermis. However, the dermal appendages are destroyed in the line of the incision and permanently lost.
2. Healing by second intention:
When cell or tissue loss is more extensive, as in infraction, inflammatory ulceration, abscess formation, or even just large wounds, the reparative process is more complex. In these situations, the regeneration of parenchymal cells alone cannot restore the original architecture. As a result, there is extensive ingrowth of granulation tissue from the wound margin, followed in time by the accumulation of extracellular matrix and scarring. This form of healing is referred to as secondary union or healing by the second intention.
Phases of Wound Healing:
The response of tissue to injury goes through several phases which are:
(a) Inflammatory phase
(b) Proliferative phase
(c) Maturation phase
(a) Inflammatory Phase:
Also called the lag or executive phase, the inflammatory phase is characterized by vascular and cellular responses that occur immediately after tissue injury takes place. The length of this phase lasts about 1-4 days. The following events occur during this phase:
1. Blood clot formation:
Right after tissue injury takes place, vasoconstriction of vessels occurs, and in an attempt to stop or control bleeding, a fibrin platelet clot forms. Lasting for about 5 to 10 minutes, this reaction is followed by vasodilation of the venules. Vasoconstriction is stopped as norepinephrine is destroyed by the intracellular enzymes. The result is increased permeability of the capillary due to the destruction of norepinephrine and the release of histamine.
2. Wound becomes edematous:
Damage of the microcirculation results in the infiltration of blood elements such as antibodies, plasma proteins, electrolytes, complement, and water for approximately 2 to 3 days after the tissue injury. This mechanism causes the occurrence of edema, warmth, redness, and pain in the affected area.
3. Phagocytes engulf debris of damaged tissue and blood clot:
The first leukocytes that move into the damaged tissue are the neutrophils. The component of WBC that transforms to macrophages to engulf the debris, monocytes, transports the phagocytized debris from the injured area. Antigenantibodies also appear and the basal cells present at the edges of the wound undergo mitosis and the resulting daughter cells migrate. Through this activity, the secretion of proteolytic enzymes and their breakdown at the base of the clot is made possible. Thus, the break in the continuity of the cells is progressively bridged and by about 24 to 48 hours the sides of the wound would eventually meet.
Hyperplastic bone marrow activity enhances cell migration progressing to the next phase of wound healing.
(b) Proliferative Phase:
The proliferative phase also called the fibroblastic or connective tissue phase, is the time where fibroblasts are multiplying and a lattice framework is formed for migrating cells. The proliferative phase occurs during the 5th to the 20th day after tissue injury took place. The following events are noted during this phase of wound healing:
1. Granulation tissue forms:
By this time, epithelial cells form beds at the edges of the wound. These beds are the ones that develop into capillaries. These capillaries serve as the nutritional source for the new granulation tissue.
2. Collagen production:
The primary component of replaced connective tissue is collagen. It is the fibroblasts that initiate the synthesis of collagen and mucopolysaccharides. Chains of amino acids convert into fibers of increasing length and diameter in about 2 to 4 weeks. The formed fibers become a well-structured pattern of packed bundles. Collagen synthesis causes depletion in the number of capillaries.
(c) Increased wound tensile strength:
Synthesis of collagen and lysis of capillaries results in the increased tensile strength of the wound. About 3% to 5% of the original skin strength is the amount of skin present 2 weeks after the injury. About in a month, only 35% to 59% of wound strength has been reached. Nevermore than 70% to 80% of the strength is regained after the wound has occurred. Vitamin C aid in the metabolic process necessary for wound healing.
Make sure you also check our other amazing Article on : Adaptation